Community Care is Cost-Effective Care

At ECHO, we pride ourselves on delivering the highest quality care in an cost-effective manner. But what exactly does that mean? Below are answers to some of the common questions that people may wonder about when determining the best option for care.
Is the cost of cancer care the same wherever you go?
No. There are several factors that influence the cost of care. This includes whether a physician practice is owned by a hospital, insurance coverage, and/ or additional fees that are charged above and beyond the cost of care.
At ECHO, we know that every dollar matters. That is why we are upfront about the cost of care, work with your insurance provider to help facilitate coverage, and do not include additional fees. Our billing department is available to help patients understand costs and we work hard to ensure that there are no surprises.
What does the term “facility fee” mean?
You may have heard this term before. A facility fee is a charge that you may have to pay when you see a doctor at a clinic that is not owned by that doctor. Facility fees are charged in addition to any other charges for the visit. Facility fees are often charged at clinics that are owned by hospitals to cover the costs of maintaining that facility and cover overhead costs, such as equipment, space, and support staff. Sometimes these are not referred to as facility fees and may have a different name.
If you have a procedure at a clinic that is part of a hospital, there may be a higher or additional charge that goes to the hospital. If you were to do that same procedure at a practice that is not owned directly by a hospital, you would not incur this fee.
Sometimes, you may not realize that there are additional charges until you are billed after the fact. Also, these costs are not always covered by insurance.
Does ECHO charge these added fees?
No. ECHO is an independent practice that is not owned by a hospital. Even though we are located within Backus Hospital, we are not owned by them. Therefore, we do not charge a facility fee, which means you may receive the same service at a lower cost.
For example, we now perform electrocardiograms in our office. If this same procedure was done in a hospital setting, the cost would likely be 2-3 times more.
Are costs of medication and chemotherapy the same everywhere?
No. Research has found that the costs of medications, including chemotherapy and infusions are dramatically higher in hospital settings and hospital based practices. Take a study published in Health Affairs: Price Differences To Insurers For Infused Cancer Drugs In Hospital Outpatient Departments And Physician Offices. The study found that the prices paid by Blue Cross Blue Shield health plans in hospital outpatient departments were DOUBLE those paid in physician offices for biologics, chemotherapies, and other infused cancer drugs (99–104 percent higher) and for infused hormonal therapies (68 percent higher). Shifting cancer infusion care to non-hospital settings, provides a large cost savings to insurers that can translate into big cost savings for patients.
What other costs may be dramatically higher?
In a 2024 comparison, ECHO found that costs across the board may be higher in a hospital setting. For instance, transfusions may cost up to 8 times higher in a hospital setting. Blood work may cost a patient 6 times more in a hospital setting. And even replacement of vitamin and nutritional deficits may cost 3-4 times more in a hospital than in a private practice.
What if I have trouble covering the cost of care?
We know facing a cancer diagnosis can be stressful, not to mention the financial burden. Our ECHO Foundation is a unique, non-profit organization dedicated to providing support services, guidance, and education to cancer patients and their caregivers. Our goal is to address each patient’s individual needs so that no one lacks care or comfort while living with cancer.
The Foundation is funded by generous corporate, business, and individual donations. Our Foundation can help patients who require financial assistance with transportation, food, supplies, and other necessities. Click here to learn more.
What other ways is ECHO is a cost-effective choice?
We offer our patients the convenience of laboratory testing right onsite. This can lead to a cost savings compared to commercial labs.
We also have an onsite medical dispensary. This allows us to provide prescriptions at a comparable or lower cost, with added convenience. A new analysis from America’s Health Insurance Plans found hospitals are charging double for some drugs they acquire and administer, while those dispersed via specialty pharmacies may serve as a more affordable and safer option for patients.
What are other benefits of a private practice?
Private physician practices are not as common as they once were, but a private practice is still your best bet for receiving the highest quality care at the lowest cost.
Independence leads to the best care. Under the private practice model, doctors have full autonomy to make the decisions that will lead to the best outcome for the patient. The trusted doctor-patient relationship is comprised of just two parties: the physician and the patient.
A third party is often introduced to this relationship when physicians work for large hospitals or health systems. These health systems, primarily led by executives, have a surprising amount of influence in the medical decisions a physician is allowed to make.
Additionally, independent practices are much more nimble than large health systems or hospitals, which means that we can adopt new technology and techniques more quickly.
Cost should not be the deciding factor when it comes to care. But it is a consideration. It is important to go with doctors you trust, in a practice that treats you like a person and has all the services you need in a welcoming environment. At ECHO, we are proud to provide this superior level of care while also remaining focused on making it affordable and convenient.
Below are some helpful articles that highlight the financial benefits of community care. Research has shown that there are many tangible cost savings that community practices deliver over hospital-based settings.
Private Practices Lead to Measurable Benefits
As the leading independent private hematology/oncology practice in Eastern CT, ECHO prides ourselves on delivering the highest quality care in a cost-effective manner. Don’t take our word for it, see what the latest research has found.
In 2023, a leading healthcare consulting firm, Avalere, was commissioned to conduct a study of Medicare spending and healthcare utilization across four physician practice models in five medical specialties (cardiology, gastroenterology, medical oncology, orthopedics and urology). In September of 2024, the first-of-its-kind study was made public.
Key findings from the Avalere study include:
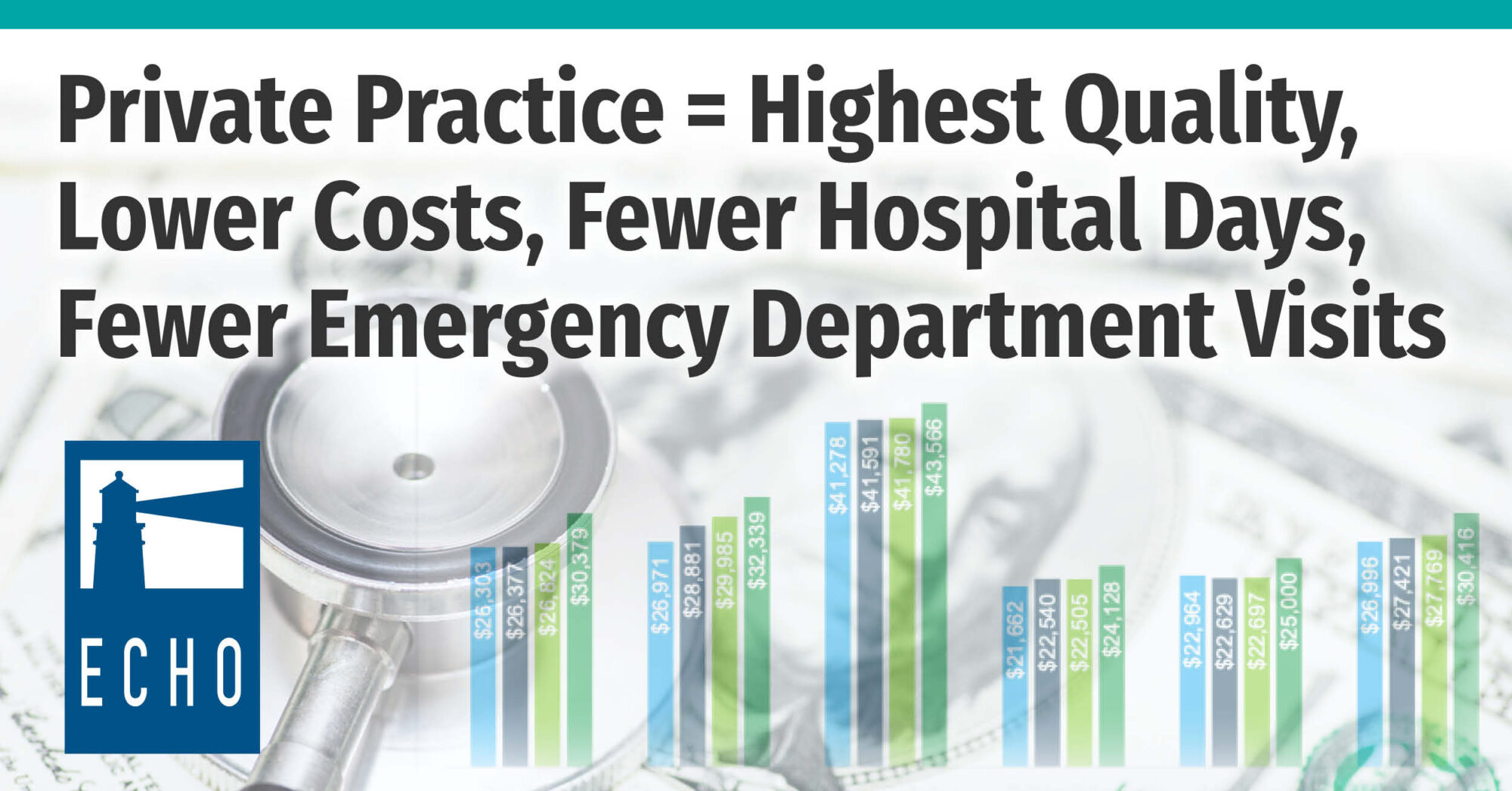
- Medicare expenditures for beneficiaries in private physician practices affiliated with private equity were, on average, 9.8% lower than for similar patients in hospital-affiliated practices in 2022.
- Beneficiaries in private equity-affiliated practices had, on average, 13.5% fewer days in the hospital and 7.9% fewer visits to the emergency department than similar patients in hospital-affiliated practices.
- Across the five medical specialties studied, per-beneficiary Medicare expenditures for beneficiaries whose physicians moved from unaffiliated private practice to a private equity affiliation were on average $963 lower in the 12 months following the transition.
- By contrast, per-beneficiary Medicare expenditures for beneficiaries whose physicians moved from unaffiliated private practice to corporate affiliation across the five specialties were on average $1,140 higher in the 12 months following the transition.
- Medicare expenditures for beneficiaries whose physicians moved from unaffiliated private practice to hospital affiliation across the five specialties were even higher — $1,327 per beneficiary higher on average in the 12 months following the transition.
This study illustrates that what independent physicians have long maintained – that private practices provide high-quality care at lower cost than our physician colleagues who are affiliated with hospitals or vertically integrated insurers. Private practices are good for our healthcare system and ultimately benefit patient care.
Community Oncology Is a Low-Cost, High-Quality Option for Care
Having the option of receiving care in their community instead of a large hospital located hours away is not only a benefit for many patients, but research is showing community oncology practices are a low-cost, high-quality provider of care. Dr. Jeff Patton, executive chairman of Tennessee Oncology and CEO of OneOncology discusses why community practices are uniquely suited to meet the needs of patients.
How will hospital price transparency impact community oncologists?
I hope that the pricing transparency shines a bright light on what we already knew, which is to show the payers in the world that we are the low-cost, high-quality provider, and that hopefully, that will allow a steerage of patients our way and really drive our businesses and help us thrive.
We now have data to prove it that community oncology is the high-quality, low-cost provider. Just a couple weeks ago, an article published about the 340B hospitals and the transparency, and they’re marking up those discounted prices as much as the other acute care hospitals.
I hope that transparency drives payers to have better conversations with us and hopefully stops the mass exodus of community oncology to hospitals and allows physicians that want to come back and practice in the community the opportunity to do so.
What’s the role and benefit of a community oncologist versus a big medical center?
For me, the primary thing is that we’re able to deliver care at a convenient place close to where patients live, instead of in a hospital campus where it’s, you know, hard to park. In Tennessee, we go out to rural areas an hour outside of Nashville, and it’s just mom and pop, and we’re delivering care right there in the community where patients are in a very convenient location. That’s one.
Two, as independent oncologists, we own our practice, so we get to make our own rules and we’re very nimble, and so we can adjust to changes in both care and care patterns, and the regulatory environment. And so, the independence of owning your own practice and providing a more convenient location for patients, to me, it’s a lovely combination.
Other than COVID-19, what is the biggest challenge facing community oncologists right now?
I think it’s always, you know, worried about what the government’s going to do. There are unintended consequences, just like 340B, I think has ballooned into something it shouldn’t have. And it’s pushed physicians toward hospitals, which is a more expensive site of service, which we now have proof of. So, I don’t worry about the government doing things, you know, against us, I worry about them doing things that have unintended consequences. And so, there are a lot.
Now the cost of cancer care is exploding, and they want to do something—I just worry that they’ll do something that’s not right for community oncology. And I know that patients deserve the choice of either been cared for in their communities, where they live, or going to a large hospital in a large city. That should be their choice, but I think they should have that choice instead of, unfortunately, the wrong law could push the world such that we can’t practice independently, which would be a shame.
To learn more and watch a video, click here.
Source:
Dr Jeff Patton Outlines How Community Oncology Is a Low-Cost, High-Quality Provider – American Journal of Managed Care, September 24, 2021
Price Differences to Insurers for Infused Cancer Drugs in Hospital Outpatient Departments and Physician Offices
The prices paid in 2019 by Blue Cross Blue Shield health plans in hospital outpatient departments were double those paid in physician offices for biologics, chemotherapies, and other infused cancer drugs (99–104 percent higher) and for infused hormonal therapies (68 percent higher). Had these plans excluded hospital clinics from their networks, channeling all of the infusions to physician offices, they would have saved $1.28 billion per year, or 26 percent of what they actually paid. Had they relied on cost-sharing incentives to channel infusions to physician offices—with either uniform 20 percent coinsurance or reference pricing—they would have realized savings but increased the financial burden on patients who received care at the higher-price hospital clinics. Under 20 percent coinsurance, patients’ payment obligations for care at hospital clinics would have exceeded those for care in physician offices by a median of 67 percent for biologics, 72 percent for chemotherapies, 87 percent for hormonal therapies, and 75 percent for other cancer drugs. Large savings are potentially available to commercial insurers from shifting cancer infusion care to nonhospital settings, but cost-sharing burdens could become very high for patients.
Source: https://www.healthaffairs.org/doi/abs/10.1377/hlthaff.2021.00211?journalCode=hlthaff
Cost of Cancer Care in the Outpatient vs Community Oncology Setting
Zack Bessette, assistant web editor for Journal of Clinical Pathways is joined by his colleague, Cameron Kelsall, associate editor of the journal. Their guest is Lucio N. Gordan, MD, medical director in the Division of Quality and Informatics at Florida Cancer Specialists and Research Institute. Dr. Gordan recently served as the lead investigator of a report for the Community Oncology Alliance titled, “The Value of Community Oncology – Site of Care Cost Analysis.” In said report, Dr. Gordan and colleagues found that cancer care is significantly more expensive when delivered in a hospital outpatient setting compared with a community oncology practice.
Below is an interview where Dr. Gordan shares some of the details of the report and the implications this cost difference have for patients.
Dr. Gordan, can you talk about the differences in cancer treatment based on site of care referenced in your report?
In our study we analyzed about 6,000 patients with breast cancer, lung, and colorectal cancer in the community setting versus hospital setting. And in our study, we did matched analysis to take out any confounding factors. We also looked at several different specifics, either demographics of the community setting versus hospital setting, including comorbidity scores, just to make sure the patients in the community or the hospital were sicker or vice versa. So, we showed our patient population of about 6,000 patients or more were very equalized in terms of the demographic features.
In our study we were able to show that in general, we are able to save about $8,000 per member per month in patients treated with breast, colorectal, or lung cancer. We also were able to show that patients in our study treated in the community setting saw the emergency department at 72 hours post-treatment at 28% less than the hospital setting. At the 10-day mark, emergency room visits were about 20% less in the community setting. So, I think these are very important findings.
What are some of the drivers of increased costs for patients treated in hospital outpatient settings?
Several things. The most important element is the cost of chemotherapy in the hospital-based practice. It’s usually at least 100-150% higher. So, unfortunately the hospital setting, the mark-up of the cost of chemotherapy, either branded or genetic agents or combination regimens is at least 100% higher. So, this is driver number one.
Number two, physician visit costs are quite higher, about fourfold to fivefold
depending upon which cancer one is analyzing for the hospital-based practice versus the community, so community practice physician visits are less expensive, probably because of less, the lack of hospital fees and others make things much more expensive.
There are other elements that make the cost higher in the community-based practice. If you compare radiation costs, the, inpatient visit, emergency room visits, comparing community versus hospital, hospital is much more expensive beyond any statistical doubt.
Do you believe financial toxicity to be a growing concern for patients with cancer? Who or what is responsible, and what are some ways of minimizing toxicity for this population?
Excellent question. As you know we have a growing older population. The incidence and prevalence of cancer will continue to rise. We have more people on treatment because our treatments are getting more effective and so patients stay longer on treatment. And the cost of some of these treatments are quite expensive and so this adds to the problem.
However, I think a very important issue pertains to the existence of the 340B program, so 340B was an idea that was initiated several years ago and the idea was good initially. It was to try to provide lower cost of chemotherapy and anti-cancer treatments for patients who are under-insured or not insured or uninsured. But the problem is that about 50% of the hospitals in the United States are under 340B programs so they’re able to buy the chemotherapy at a substantial discount of 50% and unfortunately, most of these hospitals do not offer any charity care whatsoever. So what happens is that hospitals on 340B will just enrich themselves and what happens, they’re able to build new buildings, to buy clinics, to control the market by buying internal medicine groups, family practice groups, other specialties. So, they choke the referral source to other oncologists that are not yet hospital-based. So what happens, there is almost an inevitable transfer of work force from the community setting to the hospital setting. So this lack of equilibrium in the market caused by the unintentional result of 340B really is, in my opinion, one of the most important triggers of this rise in cost of care in the hospital-based setting.
The other thing, there’s a very interesting paper called the Moran paper that shows that the mark-up of drugs in oncology can be as high as 500%, which is absurd as compared to the price from the manufacturer. So, it’s inconceivable that the hospital system can charge 250-500% higher than the actual company which created and produced this medication and got to the market after years and years of research.
I think squeezing the market by having extra cash to corner the market is very important, and also the mark-up of, excessive mark-up of drug prices is, makes it a done deal in terms of killing access to care.
In your report, you mentioned that hospitals are increasingly acquiring community oncology clinics. What are some of the long-reaching ramifications of this?
As the hospital acquires community oncology practices by choking their existence, by controlling referral patterns, for instance, by creating bigger buildings, by investing very heavily in marketing causing a terrible asymmetry in the market, we diminish number one, diversity in the community, so communities that had one or two or three clinics that are non-hospital-based don’t exist anymore. In the smaller community areas or rural areas, access to care has been very difficult to non-existent so patients are having to drive 50-100 miles to a hospital now because their oncologists do not exist any longer. They got acquired and the clinic got shut down. So we have an importance of decreased access to care, decreased diversity, lack of support of the community, and fourth is significant increase in cost. And this is unsustainable, Zachary. There’s no way to maintain cost of care in the hospital setting which is at least 100% higher as compared to the community, for no benefit in terms of quality that it can be proved.
What steps need to be taken for hospitals to lower their prices on cancer care?
They will probably not do this voluntarily. This is too good for the hospitals, to be honest, to lower the mark-up or to get away from 340B, or to use 340B appropriately. So, the only way that I see this changing is number one, legislative changes, so Congress people being more aware of the situation and changing the laws. So, this will be step number one.
Number two, educate the audience including patients, tax payers, the oncology work force, ourselves, to support what is more cost efficient and to support community settings over hospital-based settings. But it will probably take the law to really change, to enforce such changes. Otherwise, I don’t think this will happen spontaneously whatsoever.
Are there any other important points you would like to make for our audience?
Yes. I think our study again underscores the importance of community oncology staying strong and alive. We do appreciate the hospitals. They have absolutely a place in healthcare. We are supportive of the hospitals for the right reason. We need inpatient care and procedures that are necessary to be done in house. But as far as patient care in the outpatient setting, this belongs to the community. This belongs to practices that have existed forever and now they are getting out of the market pushed by unfair market asymmetries as I said before.
If our population, ourselves, want to have diversity in care, want to have better access of care, and desire to have lower costs and improved efficiencies, they need to support community oncology. As is, we have seen hundreds if not thousands of practices being closed over the last ten years, and the cost has just simply gone up and, for instance, Medicare is probably paying in excess of $2.5-3 billion a year in cancer care alone just because of the shift from community to hospital, and this is not counting other subspecialties that are also, like rheumatology that uses more expensive drugs to treat the patients.
I think as I said, the hospitals have a significant value in healthcare delivery, but something has to give in terms of the mark-up of the drugs, as well as what they can charge and receive from 340B.
Source:
Journal of Clinical Pathways; July 19, 2022
https://www.hmpgloballearningnetwork.com/site/jcp/cost-cancer-care-outpatient-vs-community-oncology-setting
Patients Benefit for Choosing Cancer Care at a Community Cancer Center
Below is an article from the Urology Cancer Center and GU Research Network about how community care is the backbone of cancer care in the United States. The article discusses the two places to receive cancer care – Hospitals & University Based Centers or Community Cancer Centers. Below are some questions and answers on this important topic.
Who cares for more cancer patients in the U.S.?
This may come as a surprise that 80% of U.S. cancer patients receive their cancer care in Community cancer centers.
Community cancer centers are Independent and NOT affiliated with a Hospital or University. Community cancer centers are often closer to home, more convenient, more personal, and more likely to offer all of your services under one roof by a smaller group of staff that are all working as one team. Community cancer centers are definitely more cost effective for patients and society.
FDA APPROVED TREATMENTS & CLINICAL RESEARCH
Community cancer centers are able to provide the same FDA approved standards of care and often sooner given their ability to more efficiently have their staff obtain insurance authorizations and financial coverage. Furthermore many community cancer centers are able to offer MORE cutting edge and innovative Clinical Research Trials than even University based cancer centers that are bogged down with bureaucracy. It can often take a Hospital or University based cancer center a year or more to open the same clinical trial that it would only take a matter of weeks for a Community cancer center to open and start accruing patients to the same trial. Some patients don’t have time to wait!
MORE CONVENIENT
Community cancer centers are typically closer to home or in your community. That allows more family and friends access to joining you for your appointments. Community cancer centers are smaller making life easier for a cancer patients that are already dealing with so much. Patients don’t need to park in a parking garage and end up lost in the vast hallways of a hospital and asking staff that they have never met for help. At a community cancer center, patients will park outside the front door, walk in, and be greeted by the same staff and smiles that have greeted them since they started as a patient. The entire staff knows that patient and is working as a team under one roof to make that patient’s experience less stressful. Your physician visit, labs, scans, prescriptions, financial help, and cup of coffee are all in the same office.
COST SAVINGS TO SOCIETY
Community cancer centers and Hospital/University cancer centers do NOT cost society the same for the exact same treatments. As a 2020 example, a patient received a drug called Avastin at UCC which cost UCC around $7,500 to purchase the drug from a pharmaceutical wholesaler and Medicare paid UCC for the drug and to administer the drug approximately $8,000. The same patient later received the same drug and dose of Avastin at an Omaha Hospital and Medicare was charged $40,000 for the exact same treatment. Much of the U.S. financial crisis is due to rapidly rising costs of healthcare, especially expensive cancer treatments. Unfortunately, more hospitals are attempting to acquire Community cancer centers which only drives the cost to society higher. Since 2008 over 700 Community cancer centers have been acquired by Hospitals.
Source:
Patients Benefit from Choosing Cancer Care at A Community Cancer Center! Community Cancer Centers: The Backbone of Cancer Care in The U.S. – Urology Cancer Center and GU Research Network